The Link Between Myofascial Pain and Headaches
The Link Between Myofascial Pain and Headaches

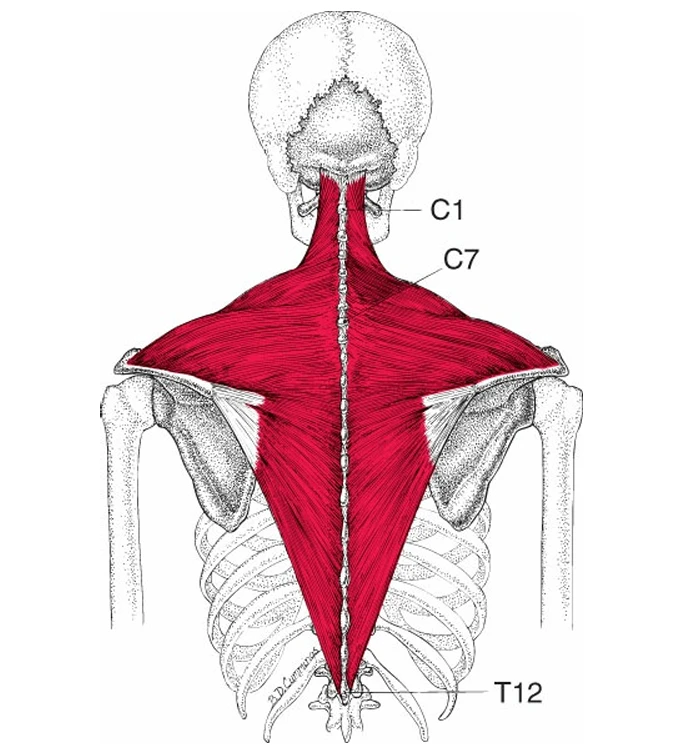
Understanding Trapezius Muscle Pain
The trapezius muscle is a large muscle that covers the back of your neck and shoulders. It helps you move your neck, head, and shoulder blades.
This muscle has three parts:
- Upper part: helps lift your shoulders and move your neck
- Middle part: helps pull your shoulder blades back
- Lower part: helps move your shoulder blades down
Why It Hurts
The trapezius muscle often develops tight knots called trigger points. These knots can cause pain in different areas:
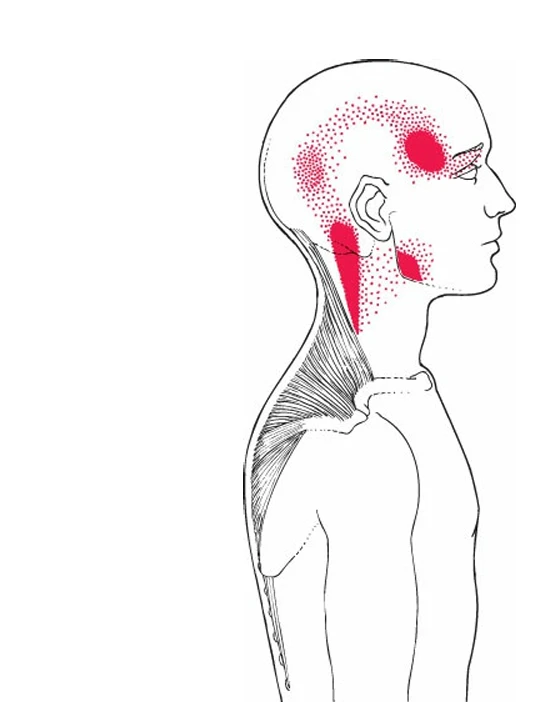
- The upper part can cause pain that spreads up the side of the neck to the head and behind the eyes — this may feel like a tension headache.
- The middle part can cause shoulder pain.
- The lower part can cause pain in the neck or upper back.
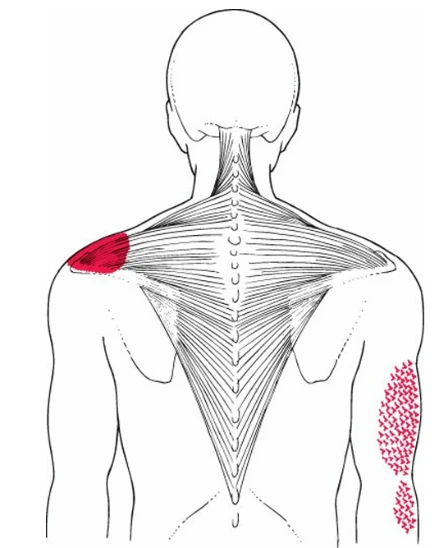
TrPs are commonly found along the anterior border of the muscle, especially in the vertical fibers near the clavicle. Pain from these TrPs typically spreads unilaterally upward to the mastoid process, and can also affect the temple, orbit, jaw angle, and, less often, the occiput or lower molar teeth. TrPs in the upper trapezius are a major source of tension-type headaches.
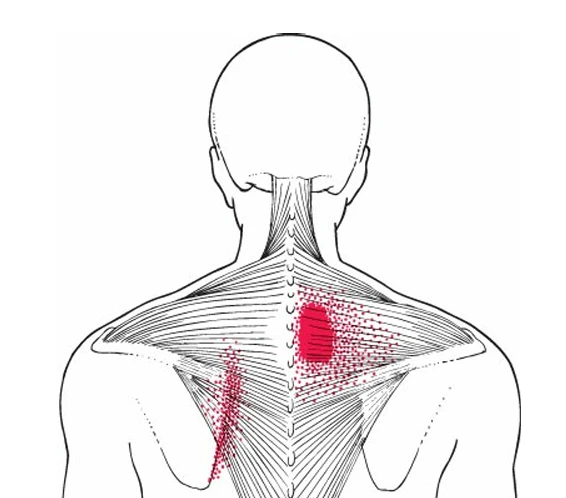
Trigger points in the middle trapezius may cause superficial burning pain between the medial scapular border and C7-T3 spines. This reported burning sensation should not be confused with pain of cervical origin, which can also refer to this area. They can also refer aching to the top of the shoulder near the acromion, overlapping with lower trapezius referral patterns. Additionally, these trigger points may produce a "shivery" sensation and pilomotor erection on the lateral side of the same arm.
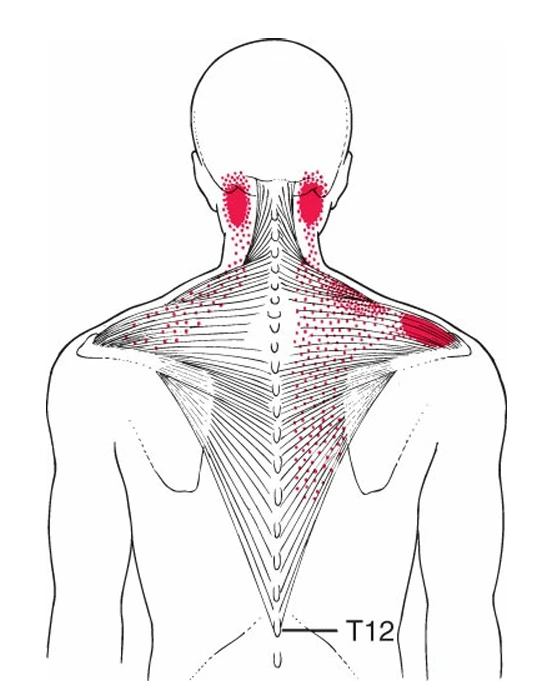
Trigger points in the lower portion of the trapezius, although common, are frequently overlooked as a source of cervical pain. They have been shown to refer pain to the high cervical region of the paraspinal muscles, adjacent to the mastoid (back of the ear area). The muscle can also refer pain to the acromion and over the suprascapular region. Trigger points in the muscle closer to the attachment on the scapula can refer a burning pain along and medial to the medial border of the scapula. This reported burning sensation should not be confused with pain of cervical origin, which can refer to the same area.
You might feel:
- A stiff neck
If a TrP in trapezius muscle is combined with the presence of other muscles including the levator scapulae or splenius cervicis, the patient may develop an acute “stiff neck.” This painfully limits rotation of the head toward the same side, which elongates the upper trapezius muscle
- Headache
With entrapment of the greater occipital nerve as a sequela to prolonged activation of upper trapezius muscle TrPs, patients report numbness, tingling and burning pain in the scalp over the ipsilateral occipital region (“occipital neuralgia”) in addition to headache
- Pain or tightness in the neck and shoulders
- A feeling of shivers or tingling down your spine
Common Causes
- Poor posture, especially when sitting at a computer for long periods
- Sudden jerks or injuries such as whiplash from an accident
- Falling or lifting something awkwardly
- Sleeping in an uncomfortable position
What Else Could It Be?
Sometimes trapezius pain can be mistaken for:
- Tension or migraine headaches
- Jaw joint (TMJ) problems
- Neck joint issues
- Occipital neuralgia (pain at the back of the head)
- Shoulder impingement
What You Can Do
- Check your posture – keep your screen at eye level and shoulders relaxed.
- Sleep comfortably – use a supportive pillow, avoid sleeping on your stomach.
- Avoid heavy bags or activities that strain your shoulders.
- Gently massage or press on the sore spots to release tension.
- Do simple neck and shoulder stretches regularly.
See a pain specialist when you don’t get relief, so how do we treat them?
- TRIGGER POINT RELEASE INJECTIONS:
Often chronic MTrPs are difficult to treat and can be inactivated by inserting a needle into the trigger zone or point (Dry needling); done by a Best Pain Specialist doctor in T.nagar in under Ultrasound image guidance.
This can be done with injection of local anaesthetic.
Properly done, a local twitch response will occur, often with a momentary reproduction of referred pain, and then the taut band will relax and tenderness will diminish or disappear.
In chronic, resistant cases, Botox injections can also be considered.
2. PROLOTHERAPY
PROLOTHERAPY has emerged as a cost-effective treatment option for chronic musculoskeletal and arthritic pain. It involves the injection of a small amount of solution into multiple painful ligament and tendon insertions (enthesis), typical trigger points, as well as into the adjacent joint spaces to induce healing of the injured structures. It is presumed to work by stimulating weakened structures such as ligaments and tendons to strengthen, tighten and heal by the induced proliferation of cells.
Dextrose Prolotherapy is presumed to work by several mechanisms including a direct, an osmotic, and inflammatory growth effect. Dextrose injections below a 10% solution directly stimulate proliferation of cells and tissue without causing an inflammatory reaction.
3. PHYSICAL CONDITIONING
Ergonomic work factors and psychological stresses that may cause or aggravate trigger point formation and activation must also be addressed and corrected or alleviated.
Once trigger point pain is reduced and perpetuating factors are addressed, a physical conditioning programme can strengthen muscle, increase endurance, and perhaps reduce the possibility of reactivating the trigger points.
0 comments
Log in to leave a comment.
Be the first to comment.